





Organic Mental Disorders · 12:16pm Nov 22nd, 2013
Pretend that there's something meaningful written here.
Psychotic Syndromes
Humour Disorders
Anxiety, Dissociative and Somatoform Disorders
Personality Disorders
Eating Disorders
The concept of normality: A psychopathological approach
Organic Mental Disorders
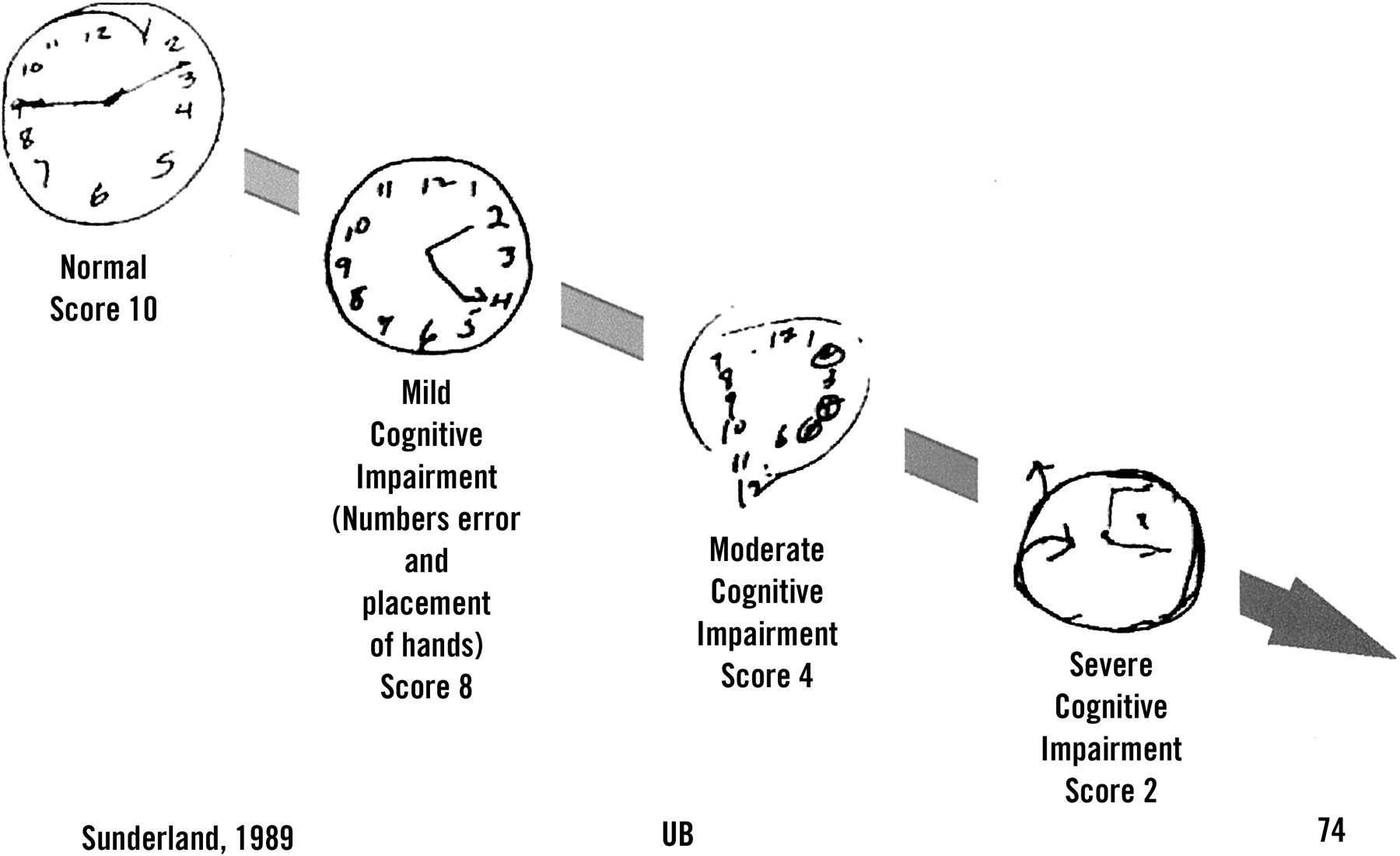
Delirium, dementia, amnesic disorder and other cognitive disorders are often grouped together into a cluster and then called organic mental disorders. Their main characteristic is the impaired cognition (for instance, memory; or language; or attention). Although a formal evaluation of the level of cognitive impairment demands a long consult with an specialist in neuropsychological testing, a practical and useful test in general clinic is the MMSE (Mini-Mental State Examination). The MMSE is a screening test that can be used in a patient's clinical examination. Other two tests that can be used are: the Verbal Fluency Test (in which the patient is ordered to name as many items of the requested category {plants; animals; everyday objects; etc.} as they can in 60 seconds) and Clock Drawing Test (in which we ask them to draw a clock at any given time {times like X:52 are used more than X:00, X;15, X:30 and X:45, due to their higher demand of a patient's cognitive functions} can evaluate the visuospatial, planning, cognitive and motor functions of a patient). The Clock Drawing Test may, sometimes, be included in the MMSE, and it is a very good method for a qualitative evaluation of a patient's cognitive impairment.
{kind=link}
I - Delirium
Also known as: acute confusional state, mental confusion and metabolic encephalopathy. It is a syndrome characterized by the global alteration of the psychic functions, manifesting itself through cognitive, attention and consciousness impairment (it can be accompanied by alterations of the sleep-vigil cycle and of the motor skills). Other psychiatric (humor, behavioral and perception alterations) or neurological (shaking/shivering and urinal incontinence) symptoms can be present as well. Classically, delirium has a sudden manifestations (hours-days), a relatively short and fluctuating course. The recovery is complete and quick, once the causal effect is identified and eliminated. It has many causes, and all of them result in a similar symptomatic pattern, related to the consciousness level and the cognitive impairment of the patient. Most causes are external to the central nervous system as, for instance, renal or hepatic insufficiency.
It is a fairly common disorder, affecting around 10-15% of patients in surgical infirmaries, 15-25% of patients in clinical infirmaries, 30% of patients in either cardiological surgery unities or intensive care units and 40-50% of patients that are recovering from a hip fracture surgery. The risk factors are: old age and preexisting cerebral lesion (for instance, dementia, a tumor, cerebrovascular disease, etc.). The presence of delirium is considered a sign of bad prognosis, with the mortality rate in one year being able to reach 50% in a year (if the cause is not removed).
Etiology
Practically every important alteration of the homeostasis can trigger delirium. The main causes of delirium are: central nervous system diseases (such as epilepsy), systemic diseases (such as cardiac insufficiency) and intoxication (or abstinence) from pharmacological or toxic agents. The main neurotransmitter supposedly involved is acetylcholine, and the main neuroanatomical area is the reticular formation. The anti-cholinergic drugs, such as amitriptyline and chlorpromazine can also trigger a delirium episode.
Intra-cranial causes
Epilepsy and post-ictal states; cerebral trauma; infections (meningitis and encephalitis); vascular disorders.
Extra-cranial causes
Drugs (ingestion and abstinence of: sedatives {including alcohol},tranquilizers, opioids, anti-cholinergic agents, anti-convulsivants, anti-parkinson drugs, anti-hipertensive, insulin and steroids); poisons (carbon monoxide, heavy metals); endocrine dysfunction (of the: pituitary gland, pancreas, adrenal glands, parathyroid glands, thyroid gland); other organs (liver {hepatic encephalopathy}, kidneys and urinary tract {uremic encephalopathy}, lungs {hypoxia}, cardiovascular system {cardiac insufficiency, arrhythmia and hypotension}), deficiency diseases (thiamine, nicotinic acid, vitamin B12 and folic acid); infections (systemic, with fever and septicemia); electrolyte imbalance (for whatever reason); post-surgery states; trauma.
Diagnosis
Delirium is usually diagnosed with the patient admitted in a clinical hospital and it is characterized by the sudden manifestation of the symptoms (lower conscience level and cognitive alterations). Using a test to see the mental state of the patient (such as the MMSE) could be useful to document the cognitive impairment in order to obtain a parameter for comparison as the manifestations progress or regress. The physical examination frequently reveals certain clues as to what caused the disorder. The history of a known physical disease, cranial trauma or alcoholic dependency point increase the chances of a diagnosis. The laboratorial investigation should always follow clinical investigation.
The impairment of conscience level and attention is mandatory for the characterization of this syndrome. Any other psychopathological manifestation can follow it. Frequently, the conscience level and the capacity for maintaining attention/focus fluctuate as the day pass. The temporal orientation is usually lost, even in light cases. The spacial orientation could be impaired in severe cases, but the auto-psychic orientation is rarely lost (the patients' capacity to know who they are). Visual and auditive hallucinations are relatively common in these patients, with the tendency to be more real and scarier. Delusions, usually with little structure, fluctuating, and with persecutory content can also happen. Humour alterations can manifest themselves as: unreasonable fear, anxiety, depression and euphoria. The sleep-vigil cycle is often impaired as well. Psychomotor alterations can also be present, be them of lentification or agitation. Very frequently, the symptoms get worse as the sun sets (an effect known as sundowning) or when the patient is exposed to excessive or scarce stimulation.
Course and Prognosis
Delirium symptoms, as their duration and their evolution, are usually directly related with the relevant causal factors. After the identification and removal of such factors, the symptoms tend to fade in one or two weeks. The patient's age and the duration of the episode could be indicative of bad prognosis.

II - Dementia
Dementia is a syndrome characterized by multiple losses of the cognitive functions, without alterations in the conscience. The main cognitive functions that are lost are, usually, memory, language, orientation, problem-solving, intelligence, perception, attention, concentration, the capacity to make judgments and social abilities. It is necessary that the symptoms result in a significant impairment in the social and occupational functions and represent a signification decline when compared to a previous level of functioning. Dementia is a syndrome and it can has many causes linked to its manifestation. Some of them are potentially reversible (15%), which makes it even more important an early etiological investigation. The main cause of dementia is Alzheimer's Disease (50-60%), followed by Vascular Dementia (15-30%).
The final diagnosis of Alzheimer's Disease is based on a neuropathological examination of the brain (though this is very infrequent in Brazil, so we adopt a clinical diagnosis after other causes of dementia are excluded). It is characterized by a demential manifestation with insidious start, usually having memory deficit as the first manifestation (in the form of simple "forgetting"s). The patient starts to forget common facts of their daily life, such as leaving the pan on a lit stove, changing objects' places and forgetting where they were, etc. The language can also be altered, evident in the name-switching for objects. Disorientation can happen, usually in time-space at first, but becoming an auto-psychic disorientation in more advanced stages. As the disease progresses, the patient becomes dependent of others to help them on their basic life tasks, such as shopping and, after some time, self-hygiene and feeding. In late stages, there can be loss of sphincter control, leading to urinary and fecal incontinence, dysphagia and seizures.
Also: You might think I was fucking with you when I said that the patient needing to draw a clock is counted as an important test.
You'd be wrong.

Seems about right. You're just a textbook waiting to be fed through a printing press, aren't you?
...
Hrm... wonder what would happen if I drew this in my clock test.
i.imgur.com/CJsrmyQ.jpg
Probably be shot on sight in several countries. Heh.
1531571 Well, I do study like an unfed, constantly-whipped slave for internship. At least that has been working.
Now that I think of it, internship is the evolution of slave labor. I'm paying them... TO WORK FOR THEM!
I wonder how long we have before Apple discovers this disturbing view...
At best, you'd get some weird looks, though I don't yet have an educated opinion on sexual perversions (ya, this is how it'd probably be called), so I'll refrain from commenting in order to avoid vomiting bullshit.
Though, personally, I have nothing against pony butts. Nor I have anything in favor of them (except Rarity's).
1532231
Wooo~ Perversions. That's this site's bread and butter. And honestly, I think every company ever does that slave labour thing you have to pay for. I think they market it to masochists.
i.imgur.com/caC36mI.gif
1532844 Ah, yes... this site. I can't fault the authors/stories around here; they basically cater to their readers' tastes. Though so much time has passed since something good has been posted [that I have noticed] that I often wonder why is it that I stick around. To be honest, basically nothing around here brings me joy/fun/happines/whatever anymore. It isn't a bad experience; it's just not fulfilling anymore.
(No, not even these informative posts. And I am starting to think that I'm doing more bad than good by allowing them to say. The error's been committed, though; I won't erase them and try to deny it.)
I reckon I should just finish Dysphoria and be done with the world of Meine Kleines Pferden: Hugfriend is Wizardry fan fiction. It's not like I'm losing anything anyway.
And don't even get me started on it. I don't even have a job and I'm already scared shitless of working.
Now, if you excuse me, Muzz, I think that, since this is the internet, it is in good measure that I say these next words. They are now targeted towards you, mind.
A reasonable warning to any motherfucker trying to extrapolate on my words and take them out of context: When I say that nothing good is on this site anymore, I mean it with all the weight of my subjective perspective. No, I am not calling you/your writers/your stories stupid. I am stating that I don't like them. I am not stating that they are shit. I am stating my personal opinion, which should only be taken by heart by myself and myself alone. No, I do not hate you for liking them. No, I do not think less of you for liking them.
Though you, eventual reader, probably deserve to be called an idiot if you are the kind of person this warning is targeted to.
1548119
You have a good point. Its been months since I've seen something that was truly entertaining, and its been AWOL for just as long. I have one last foray to delve into with my fictions, and then I'm done. I'll have told my story. I don't plan to ever even post it until its a perfected work. Then I'll post it sequentially, and that'll be it. It will be harsh, unforgiving, and bitter. Hopefully you'll still be here when its done. I enjoy reading your informative posts, and I keep them close at hand should I ever need to refer to them. Every time you make a post, I can pretend for a moment its still the old days.
Meanwhile: in the Lightning Sphere. Running into server expansion issues, but we've had a massive influx of popularity. I'm getting better at management and commentary, my staff is loyal and hard working, and my audience is adoring. Maybe I've found something I enjoy doing.
1549090 Ach, ja, der alten Zeiten...
I seriously doubt I'll still be here, Muzz. Unless you can get everything wrapped up before December ends, that is. The general quality of stuff has decreased and, while I'm not going to hold the author guilty, my own interest diminished as well. Nearly everything is overdone; which isn't a bad thing per se. But the way stories are constructed gives little room for appreciation, as it tries to go toward wish-fulfillment--something that is hard to notice, but it's there--and unreal social situations.
Then again, as Owlor puts it; I shouldn't complain about a pet store selling more cat food than goat food. The authors merely cater to their audience. And, who'd guess, it works!
I am glad that you like my blog posts. At least they weren't a complete waste of time. I'm considering doing a final one about substance abuse on Thursday, if everything goes according to plan (my humour included). But what I want, after classes are over, is to finish Dysphoria and just be done with fandom!pony completely. I'll most likely still watch the episodes and read the comics (the comics are really good, btw).
Even though Dysphoria is... about 85-90% completed, it still needs editing (and our editor suddenly disappeared; I hope everything is alright with him) and the last 3 chapters still need to be written. I will most likely write it and bail, leaving Owlor to either edit it by himself or find an editor. I've written enough as is, but I promised that I'd finish writing it.
I'm a tired asshole who needs to move on with his life already and focus on my future a bit more than I already am (though 80% of my time is spent toward said cause; I personally think that it is still insufficient). I will pop in on Skype to chat sometimes; but as I get nearer and nearer to internship, less and less time will be spent doing other things other than focusing on my graduation.
After I'm graduated, who knows? Maybe I'll be back.
PS: This arena thingymajigger sounds a lot of fun. I wish I had time/computer specs to play. I really do.
1564467

Bit of shame, then. Oh well. I'll just link it in skype or something. Its likely it won't be done for another year or so, so maybe you'll stumble over it when you're graduated. I'll find something one day that could match up to the works of olden-times. Maybe. Probably.
...
I'll get the alchemy books out, and we'll see if we can turn this shit into gold.